Provided by: Roger Friedman, MD (Allergist/Immunologist)
This is a unique and challenging time for all of us! A question I often hear is, “Could this be COVID-19 or is it my allergies?” First of all, allergies, asthma and COVID-19 do have some similar symptoms, including a runny nose, sneezing and cough. Allergies will often also cause itchy nose, eyes and throat; COVID-19 does not. In addition, most allergy sufferers know they are allergic to the tree pollen that is currently out, so their symptoms will be worse after being outside.
With COVID-19, patients will often have a fever which doesn’t occur with allergies. The sudden loss of the senses of smell and taste is a newly discovered symptom of COVID-19.
I have given you a few helpful ideas but if you’re worried or unsure please call us, we are all available! With your safety in mind, we have found new ways to care for our patients. (IE: phone calls and/or telemedicine) Request an appointment at OhioENTandAllergy.com today!
Everyone deals with a sensation of a stuffy or blocked nose from time to time. Usually we know why this is happening—we may have a cold, springtime allergies are here, etc. We are designed to breathe through the nose. It is uncomfortable to us to feel a sensation of congestion. This can also affect our sense of smell and our ability to appreciate flavors. Chronic mouth breathing over a long period of time can lead to dental problems. And for children it can lead to misalignment of the teeth and they can develop bite problems. Nasal congestion can contribute to snoring and sleep apnea as well.
Sometimes nasal blockage or congestion becomes more recurrent or chronic or its cause is unknown. This will be a brief discussion of a variety of things that can cause nasal congestion, how they are diagnosed and treated and which may be serious enough to require a trip to your PCP or even a specialist.
Basic understanding of the nose and sinuses
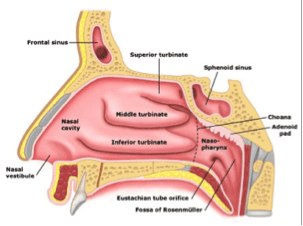
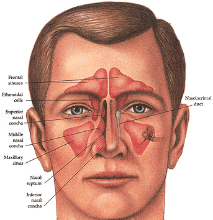
Knowing the parts of the nose helps to understand what can occur to cause blockage of the nasal passages.
The nasal passages provide filtration, humidification and warming of inhaled air on its way to the lungs. The nasal septum divides the nasal passages. It is usually fairly midline. If it is off of the midline it is referred to as a deviated. Most people have a slight deviation of the septum. The nasal turbinates are natural swellings in the nasal passages allowing for heat exchange, humidification and filtering of the air. Filtering occurs by particles sticking to a thin layer of mucus which covers the nasal turbinates. This mucus is produced by the sinuses. The mucus is constantly in motion, being swept to the back of the nasal passage by tiny fibers called “cilia” and into the throat where the mucus is swallowed. Particles are trapped in the mucus, including bacteria and viruses which are killed in stomach acids. The adenoids are located in the back of the nasal passage. They contribute to the immune system in children but can pose problems if they become too large.
Here are some of the common causes of nasal stuffiness
Acute upper respiratory infection (“common cold”)
The cause is a viral infection. One of many hundreds of viruses can cause this. The many types of viruses is why we don’t become immune to every virus and we continue to get colds every year. These are more common in the winter months when we are confined indoors and can more easily spread the virus which is passed around by direct contact or droplet spread from coughs and sneezes. Adults usually get 2-3 colds per year and younger children can get 6-10 per year as their immune systems are developing.
Symptoms include, scratchy or sore throat, cough, runny nose and sometimes low grade fever. The nose is congested because of swelling of the nasal turbinates and excessive mucus production. Also, the viral infection damages the cilia, so the mucus does not move properly and collects. This results in runny nose, post nasal drainage and cough. This leads to further swelling and more congestion.
Treatment is intended to treat symptoms. We simply don’t have medications to treat most viruses. Nasal saline rinses (Neti pot or NeilMed® sinus rinse), saline nasal spray, OTC nasal steroid sprays (Flonase,® Nasocort®), Tylenol®/Motrin®, mucus thinners and decongestants (Mucinex® or Mucinex-D®) can all help. These treatments help to thin and clear out mucus and decrease inflammation and swelling. Decongestant nose sprays can be helpful but should not be used for longer than 3 days to prevent “rebound swelling”, making the problem worse. Other medications are available and oftentimes your pharmacist can provide excellent advice.
Antibiotics given within 10-14 days don’t usually help because bacteria are not present during this time period. Symptoms worsening after 10 days or lasting longer than 14 days can mean that a bacterial infection is present. Antibiotics can be helpful then. It is advisable that parents consult with their child’s pediatrician before starting any over-the-counter medication for the first time. This is especially true in younger children.
Warning signs: high fever, severe headache, swelling around eyes, vision change, shortness of breath. Persistent symptoms should all prompt a visit to PCP or urgent care.
Allergies or Allergic Rhinitis
Some people react to particles in the air. These particles, called “allergens” include pollen from various plants, dust, mold or pet dander. Allergies occur when the allergens are inhaled into the respiratory tract of allergic people. The particles cause cells in the nose to release histamine, which then leads to the symptoms of sneezing, running nose and nasal congestion. Some patients wheeze from asthma — asthma and rashes are sometimes related to allergies. Allergies can be seasonal or year-round depending on what the patient is allergic to.
Many OTC meds are available. These will improve most of the symptoms of allergies including congestion. These include antihistamines (Claritin®, Allerga®, Zyrtec®). Sometimes these are combined with a decongestant (with a “-D” in the name). Some older antihistamines like Benadryl® are effective but are sedating. Saline spray or rinses are very helpful to clean out the allergy particles and mucus. OTC nasal steroid sprays can be extremely effective but must be used daily to be effective. Though decongestants can help, these are not ideal for daily use as they can raise blood pressure and cause other side effects. Decongestant nose sprays are to be avoided for treatment of allergies because they cause much more harm than benefit if used over time.
Avoidance of allergy exposure is extremely helpful. For this reason a referral to an allergist for allergy testing can be very beneficial to lead to improved symptoms. There are also other prescription allergy medications which might be prescribed. Some patients will benefit from “desensitization” of their allergies with allergy shots. Stronger sprays are available by prescription. Newer “biologic” medications are now available for severe cases of allergy and asthma. These will provide benefit to the most challenging patients who may have not responded to other treatments. Always consult with your PCP before starting OTC medications for your child or yourself if you’re on other medications.
Over time, severe allergies can cause significant problems in the nose and sinuses, including the development of nasal polyps (see below). Asthma flare-ups can also become worse over time. Some people can have allergies that are so severe that they can develop life-threatening anaphylactic reactions. For these reasons, patients with allergies that are not well-controlled will benefit by an allergy evaluation. It is advisable that parents consult with their child’s pediatrician before starting any over-the-counter medication for the first time. This is especially true in younger children.
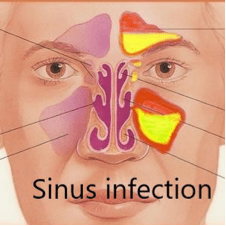
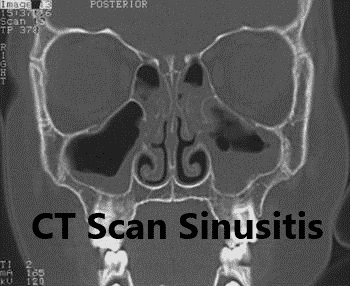
Sinus infections
Sinus infections occur when the sinuses are blocked long enough for mucus to become infected with bacteria. This can occur with a viral cold, frequent allergies or any other condition that leads to blockage of the nose. Some patients are genetically predisposed to developing sinus problems. Symptoms of a sinus infection include: nasal drainage, facial pressure, nasal congestion, cough, decreased sense of smell, ear fullness. The symptoms of a viral upper respiratory tract infection are nearly identical to a sinus infection, but more severe and last longer. In most patients, the viral cold does not progress to a bacterial infection. This is considered if the symptoms last longer than 10 to 14 days.
Treatment of a sinus infection
The same medications that help with the symptoms of a viral upper respiratory tract infection will help a sinus infection (please refer to that section above). If symptoms are not improving or if they seem severe, seeing your physician or an urgent care physician is necessary. Antibiotics or steroids (prednisone) may be prescribed. Medicated nasal rinses may be prescribed. In general antihistamines do not help unless allergies are present.
There are two types of sinus infections: recurrent infections which come and go and chronic infections which never leave.
Newer medications are being developed to treat the inflammation that contributes to the development of sinus infections in some patients. These medications are similar to medications that are used for asthma, allergies and chronic dermatologic conditions — which all have similar causes.
Surgery is also an option for patients who continue to have problems. Surgery can improve symptoms and allow for additional treatment options such as antibiotic or steroid sinus irrigations. Nasal and sinus surgery used to have “a bad reputation“. This is based on the earlier types of surgery that were performed. Most of the time today, the recovery is very manageable and nasal packing is not required.
Warning signs of a sinus infection
Sinus infections can be severe and even life-threatening. If a sinus infection is not improving or if other symptoms develop including high fever, severe headache, facial swelling, or vision change, the patient should call their primary care doctor or present to the emergency department for evaluation and treatment.
Other causes of blockage of the nasal passages
In addition to the conditions discussed above, there are a variety of conditions that can lead to chronic blockage of the nasal passage in both children and adults. Many of these conditions have familiar sounding names but are still somewhat confusing to the patient. Here are a few of those (refer to diagrams below for further information):
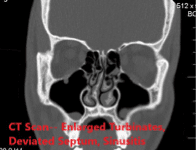
Deviated nasal septum: The nasal passages are divided by a thin piece of bone and cartilage called the nasal septum. Most patients have a “deviated nasal septum“. Minimal deviation of the septum does not cause problems and in fact may be somewhat beneficial, helping the nose to filter air. If the septum is severely off-center it can block the nasal passages and make the patient feel congested all of the time. This can also lead to the development of sinus problems. Occasionally headaches can be associated. This problem can occur after previous nasal trauma or for unknown reasons. Some patients are born with this. This problems is correctable.
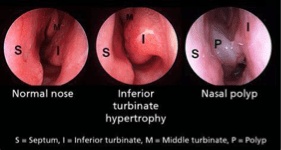
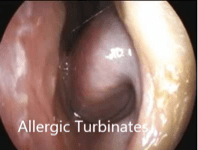
Turbinate enlargement: The nasal turbinates help those two filter warm and humidified air. They swell with inflammation from infection or allergies. Because they are very vascular, they can swell more when gravity affects them. This is why one sometimes feels more congested on the side of the nose that is toward the pillow during a cold or allergy flare-up, while lying in bed. In some cases they remain chronically swollen, requiring medical or even surgical treatment.
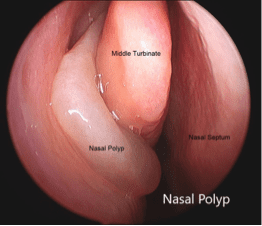
Nasal polyps: These are benign growths that occur in cases of prolonged inflammation in the nasal passages and sinuses. They can be associated with allergies or sinus infections. In some cases the cause is not known. They can become large enough that they completely block both nasal passages, leading to a vicious cycle of infection, inflammation and further polyp formation. In very rare cases polyps can be aggressive or even cancerous. Polyps can also be associated with a condition called cystic fibrosis. Any suspicion of polyps requires further evaluation.
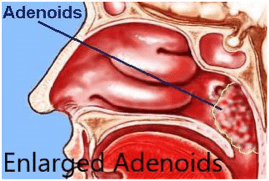
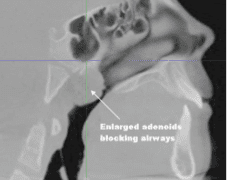
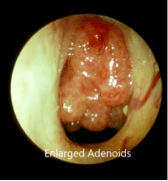
Adenoid enlargement: The tonsils and adenoids are part of the immune system. They usually quietly do their job but they can also cause problems. When adenoids become enlarged they can cause chronic nasal congestion, usually in children but sometime adults. This can lead to mouth breathing and a chronic runny nose. It can contribute to the development of dental or orthodontic problems. They can also cause blockage of the eustachian tube and lead to ear infections. Adenoid enlargement should be suspected in any child with chronic nasal problems. Adenoid enlargement in adults can be a sign of more serious problems and always requires further evaluation.
Nasal foreign body: Children are curious and will sometimes put foreign bodies in their ears or nose. If this is not witnessed, a nasal foreign body can slowly cause problems. Symptoms include chronic runny nose from one side, chronic bad breath, cough and blockage of one side of the nose. The symptoms can slowly develop and can be attributed to allergies or common cold. Patients have been seen with nasal foreign body that have been present for years in some cases. Most of the time a nasal foreign body will not cause severe symptoms but it can rarely be aspirated into the lower airways and cause significant problems, including pneumonia. Any child with persistent nasal symptoms should have further evaluation.
Nasal/sinus tumors: These are very rare. When first developed they cause typical nasal and sinus symptoms including blockage of the nose, drainage or bleeding and facial pressure. These tumors can be benign or malignant. The earlier they are diagnosed the more successful the treatment will be. Any persistent nasal or sinus blockage in adults or children should have further evaluation if those symptoms do not improve with treatment.
Overuse of nasal decongestant sprays: These sprays are very effective for short-term use, treating viral colds or a severe allergy flare-up. They should not be used for longer than 2 to 3 days. Longer use can cause symptoms of “rebound congestion”, making the original symptoms even worse. If they are used for a prolonged period of time they can lead to destruction of the tissues in the nose, including perforation of the nasal septum. This is a very difficult problem to correct.
Sleep apnea can be associated with nasal congestion. A blocked nose can lead to snoring and even obstructed breathing during sleep. Patients who have been diagnosed with sleep apnea may not respond well to usual treatment if they cannot breathe properly through their nose.
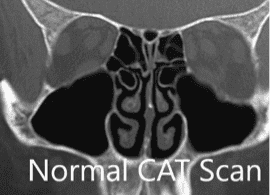
In summary, there are many conditions that can cause a feeling of blockage of the nose. The most common causes include a common cold, allergies and enlargement of the adenoids. Many of these can be treated successfully with over-the-counter medications with guidance from the patient’s primary care physician or pharmacist. Persistent symptoms should lead to further evaluation and sometimes a referral to an ENT doctor or allergist. Any evaluation and testing should allow for correct diagnosis. Testing may include a simple office endoscopy, office CAT scans, allergy testing or sleep apnea testing. These are covered by insurance. Further testing might lead to an unknown suspected diagnosis allowing more effective treatment.
Prescription medications can be very helpful. Newer medications are being developed for nasal and sinus problems as well as allergies and asthma that will lead to significant improvement in quality of life.
In some cases surgery may be necessary. These surgeries have improved significantly over the last 20 years. Post-operative discomfort is usually mild, packing is usually not required and the recovery is fairly quick. Success rates are very high. The allergists, ENT surgeons and sleep doctors at Ohio ENT and Allergy Physicians would be happy to evaluate you or a family member if any of these problems are present.
Ragweed pollen is the cause of allergic rhinitis that begins in early August and lasts until it frosts a few times, which kills the weed. Ragweed pollen is everywhere – especially in the woods, fields and in the center strip of highways. The pollen counts can be over a thousand, especially during the heavy pollination times (early in the morning and late afternoons).
The first strategy is avoidance of the pollen. You can do this by keeping the windows in the house closed and using the AC. When you exercise try to avoid early am and dusk.
We use a variety of medications to treat hay fever, including antihistamines, nasal steroids, nasal antihistamines and Singulair®. Each patient responds to these differently, so if one fails another may succeed. If these work then no further evaluation may be needed, but if patients continue to suffer it’s time to see your Allergist.
The diagnosis is usually confirmed by a visit to your Allergist where skin testing can guarantee that the proper problem is being treated. Immunotherapy or allergy shots are our most effective treatments, and can actually cure the problem.
Nosebleeds (epistaxis) are one of the most common issues seen by Ear, Nose and Throat doctors. Patients with recurrent nosebleeds have a strong desire to rid themselves of this issue, given that nosebleeds often occur at inopportune times and places and ruin clothing! The main risk factor is dryness, but the increasing use of blood thinning medication is also a strong risk factor. High blood pressure, allergic rhinitis, chronic sinus disease, nasal trauma and bleeding disorders are other possible factors.
Most commonly, nosebleeds arise from small pinpoint areas of mucous membrane blood vessel disruption, even in the case of a gushing nosebleed. You would be surprised how much bleeding can occur from a blood vessel the size of a pencil tip! You should be reassured that it is very rare that nosebleeds – even when severe – would represent any concerning intranasal process. The vast majority of nosebleeds occur on the septum, the cartilage structure that divides the nose into two passages. Nosebleeds in the back of the nose which drain primarily down to the throat are more commonly related to high blood pressure. Some of these nosebleeds can be severe and more difficult to manage.
The main treatment of nosebleeds is prevention. Consistent use of moisturizing products on the mucous membrane of the septum is key. Any number of products can be effective, including petroleum jelly and saline gel using a cotton swab. Alternatively, nasal saline spray can be used at least a few times daily. A humidifier is also advised when you have the heat on since all heat is dry. Encourage children to limit digging in their nose and moisturize scabs in the nose instead of trying to remove them.
An active nosebleed should be treated with pressure for about fifteen minutes by pinching the nostrils against the septum. Holding the bony upper nose is ineffective. Stuffing tissue paper in the nose will only pull a scab off when the paper is removed, causing the nosebleed to recur.
If a nosebleed is recurrent or persistent, then nasal cautery or packing may be necessary. An ENT physician at Ohio ENT and Allergy Physicians can often cauterize the offending source with chemical cautery using silver nitrate or electrocautery. Most children will tolerate chemical cautery in the office. If a nosebleed is profuse, sometimes packing the nose with a sponge-like material is necessary for a few days. Severe nosebleeds may need to undergo surgery or an interventional radiology procedure called embolization to occlude the blood vessel internally. The Otolaryngologists at Ohio ENT and Allergy Physicians are able to see patients with a history of nosebleeds in a timely manner to determine the best management for this troublesome issue.
Western medicine that we practice in the United States is currently based on observation, testing, diagnosis and treatment. Observation includes physical examination and a thorough history. Testing is selected based on the patient’s history and suspected causes of the patient’s problems. At Ohio ENT and Allergy Physicians, the board certified Allergist uses testing techniques and laboratory techniques that are proven to be safe and relevant, based on scientific study and published in peer-reviewed journals. Then the results, correlated with observations and physical examination, and plans of therapy are discussed with the patient.
Allergy prick skin testing is still the most physiologic form of testing for allergy. Blood tests such as RAST and Immunocap testing are helpful in that they determine if there is sensitization to a particular allergen. It must be correlated with physical and clinical symptoms. Another proven method of testing for allergies is a challenge. This can be an environmental challenge and done in research settings where patients are exposed to known allergens by breathing it in, or a food challenge when patients ingest a small increasing amounts of the food in question.
There are many other tests available. Many have not been proven to be of any clinical significance. For example, IgG4 is touted as a test for food sensitivities. However, IgG4 to foods can be found in many people who have absolutely no problems with foods. Testing for food sensitivities using IgG4 has no proven clinical benefit, and often leads to very strict restrictive diets that are totally unnecessary and may be emotionally or physically harmful.
Other tests have absolutely no basis in science. These include ALCAT testing, NuTron testing, Mediator release test, sublingual testing, provocative testing, food immune complex testing, applied kinesiology, electro-dermal testing, Neurological Stress Reduction Therapy, and laser testing and treatment. This is by no means a complete list. Many of these techniques cloak themselves in scientific jargon and claim to be cutting-edge, but really depend upon a poor understanding of physiology and science in general.
At OhioENT and Allergy Physicians, we see a tremendous number of referrals for thyroid nodules. Many times, the patients are told by their primary care physician that they need a Fine Needle Aspiration Biopsy of their thyroid nodules to determine if they are cancerous or not. We do perform many Fine Needle Biopsies the same day as their initial appointment, but oftentimes, we may defer the biopsy or bypass the biopsy and go straight to surgery. This may confuse the patients who simply assumed that it was mandatory to see the surgeon for a Fine Needle Biopsy.
I would like to educate the public on the rationale that the thyroid surgeon goes through in their mind to determine what the best protocol might be for each patients’ needs. Understanding that in general, only 5% of all thyroid nodules are malignant may put the patient at ease, but there are certain nodule characteristics that may be more alarming and raise the index of suspicion for cancer than others.
Nodules that for sure should be considered for Fine Needle Biopsy the same day as initial office visit with ENT Surgeon:
any single nodule between 1.0-1.5 cm in size (when there are not multiple nodules present in the remainder of the thyroid) that can be easily palpated or felt on exam
a large, purely cystic nodule (nodule consisting of fluid only) > 1.5 cm that can be easily palpated on exam
any single nodule on unhealthy patients whom the surgeon feels would not tolerate surgery well and would be better off monitored for nodule growth (elderly, sickly, significant cardiac/pulmonary/renal disease, etc.)
Nodules that should bypass a Fine Needle Biopsy and go straight to surgery:
any nodule > 1.5 cm (the rationale is that once nodules grow larger than 1.5 cm, there is too much sampling error with a skinny little needle which may miss a cancer)
patient with a family history of thyroid cancer
patients with a history of radiation therapy to their neck region
patients that have multiple nodules throughout their thyroid gland where any of the nodules are > 1.5 cm (there are too many nodules to biopsy)
nodules that have microcalcifications (especially if the microcalcifications are in the rim of the nodule) since this has a much higher incidence of being cancerous
nodules > 1.5 cm that are considered “complex” (contains both a solid and fluid component) since this has a higher incidence of being cancerous
Nodules that can be simply followed with repeat ultrasounds and can bypass Fine Needle Biopsy:
elderly or sickly patients (as noted above) and patients on blood thinners who would be too high risk for surgery and do not have a history of radiation to neck, family history of thyroid cancer, no microcalcifications in the rim of the nodule
single nodules < 1.0 cm
multiple nodules in the thyroid with all of them < 1.0 cm
Patients who need to be scheduled for an Ultrasound-Guided Fine Needle Biopsy through the Radiology Department:
nodules that are > 1.0 cm, but cannot be felt on exam by the surgeon
nodules that are too close to the carotid artery to be safely biopsied in the office
*These guidelines are the opinion of a thyroid surgeon with 25-years experience and should only serve as a suggestion for planned treatment – each case should be considered individually.
Pediatric Tonsillectomy and Adenoidectomy (known as a T&A) is the second most common pediatric surgical procedure performed. There may be a variety of reasons your child might be referred to one of our Ear, Nose and Throat Specialists here at Ohio ENT and Allergy Physicians.
The more common reasons to be referred by your child’s Pediatrician, Family Physician or Dentist are: chronic tonsillitis (or strep throat), snoring, obstructive sleep apnea (where your child has pauses in their nighttime breathing, breath holding and gasping episodes), swallowing problems where they appear to be choking on food, chronic halitosis (bad breath), and chronic mouth breathing which can lead to misaligned teeth.
Complications are uncommon, but fewer than 1% of children can have bleeding after surgery. Most of the time, this is self-limiting and nothing further needs to be done, but on a rare occasion, your child may need to go back to surgery to have the bleeding stopped. Most children should expect to miss 1 week of school to recover.
Thousands of these procedures are performed annually in Central Ohio. The Surgeons at OhioENT and Allergy Physicians, collaborating with the finest Anesthesiologists, have performed nearly 21,000 pediatric tonsillectomies over the past 20 years at The Ohio Surgery Center.
The Ohio Surgery Center was the first-of-its-kind Single Specialty All-Ear, Nose and Throat Surgery Center in the country. Their safety record is unsurpassed, receiving only the highest accolades from the national governing board, JCAHO (Joint Commission on Accreditation of Healthcare Organizations). Our surgeons are Board Certified and have received an extensive 5 years of tonsillectomy training of all age groups in their residencies and work alongside anesthesiologists who have also received pediatric training with Board Certified Pediatric Fellowship Trained Anesthesiologists on staff.
Ear infections are one of the most common disorders to that affect children. These can often be managed with medication without the need for further intervention. Sometimes, however, your child’s doctor may recommend that your child have an evaluation with an otolaryngologist. Below is an explanation of what ENTs are, a discussion of normal ear anatomy, and an explanation of when ear infections may warrant consideration for ear tube placement.
WHAT IS AN OTOLARYNGOLOGIST (ENT)? An ENT is a doctor who is specially trained to diagnose and treat disorders of the ears, nose, and throat medically or surgically if needed. Therefore, they are also called head & neck surgeons. It’s a mouthful to say “Otolaryngologist – Head & Neck Surgeon” therefore usually we just go by “ENT.” ENT training is quite rigorous and entails 4 years of medical school after college, followed by 5 years of residency training. Some ENTs pursue additional specialized training after residency. This extra training is called a fellowship and is usually 1-2 years in length.
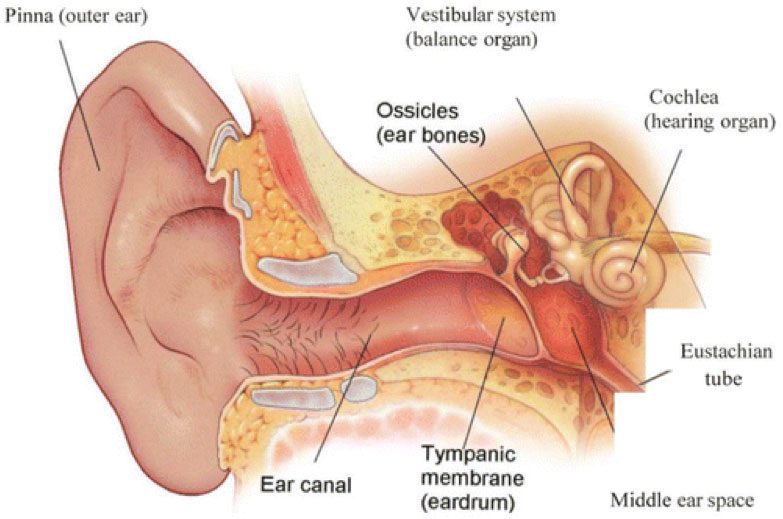
WHAT ARE THE PARTS OF THE EAR? Please see the diagram below.
Rosenfeld RM. A Parent’s Guide to Ear Tubes. Hamilton, Ontario, Canada: BC Decker; 2005. Reproduced with permission.
Outer Ear When many people think of ears, they think of the part they can see. This is called the auricle or pinna. This is the part of the ear that we can see with our naked eyes without any special instruments. This part of the ear is made up of skin that tightly surrounds a cartilage scaffolding. The bottom part of your auricle is called the lobe (or lobule), and is made up of skin and fatty tissue. This is the part of the ear that is most commonly pierced by earrings. In the center of your outer ear is a small hole called the external auditory canal (ear canal) which is a small tunnel that leads to the ear drum (tympanic membrane). Even though you cannot see most of the ear canal, this is also part of the outer ear. The ear canal is lined by skin, beneath which the outer portion is cartilage and the deeper portion is bone. This portion of the ear is where earwax (cerumen) is made.
Middle Ear The ear canal leads to the ear drum (tympanic membrane). The ear drum protects the middle and inner ear structures from the outside world. The ear drum is also connected to one of the ear bones called the malleus. The ear drum amplifies sound that is directed from the outer ear and transmits this sound to the ear bones (ossicles) which then transmit sound to the inner ear. Connected to the middle ear is a special tunnel called the Eustachian tube. This tube is primarily composed of cartilage and is connected to the muscles in the back of the throat. This tube opens into the back of the nose at the junction of the nose and throat in a region called the nasopharynx. The Eustachian tube opens and closes many times per day to allow air into and out of the middle ear space (behind the ear drum). This is the same tube that opens and closes when you ride on an airplane and feel you ears “pop.” In many children and some adults, sometimes these tubes do not function properly, and can result in Eustachian tube dysfunction (ETD). This results in the accumulation of fluid in the middle ear and is known as otitis media. This fluid can cause hearing loss, balance problems, ear discomfort, or other symptoms.
Inner Ear The inner ear is composed of a snail shaped bone called the cochlea as well as bony balance canals (semicircular canals). The third ear bone (stapes or stirrup) fits into the inner ear like a piston its vibration moves fluid in the inner ear which then creates an electrical signal that travels to the brain via the cochlear nerve (hearing nerve). Your brain then interprets this signal as sound.
Below is some very helpful information from the American Academy Of Otolaryngology – Head and Neck Surgery (AAO-HNS) regarding ear tubes (reproduced with permission). More information can be found at https://www.entnet.org//content/ear-tubes
Painful ear infections are a rite of passage for children and by the age of five, nearly every child has experienced at least one episode. Most ear infections either resolve on their own (viral) or are effectively treated by antibiotics (bacterial). But sometimes ear infections and/or fluid in the middle ear may become a chronic problem leading to other issues, such as hearing loss, poor school performance, or behavior and speech problems. In these cases, insertion of an ear tube by an otolaryngologist (ear, nose, and throat specialist) may be considered.
According to the American Academy of Otolaryngology – Head and Neck Surgery, “consultation with an otolaryngologist may be warranted if you or your child has experienced repeated or severe ear infections, ear infections that are not resolved with antibiotics, hearing loss due to fluid in the middle ear, barotrauma, or have an anatomic abnormality that inhibits drainage of the middle ear.”
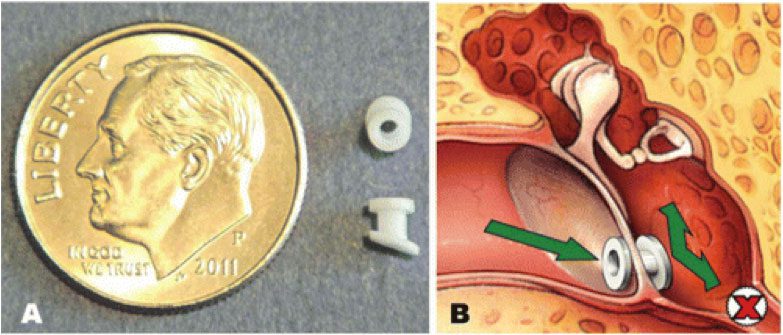
WHAT ARE EAR TUBES? Ear tubes are tiny cylinders placed through the ear drum (tympanic membrane) to allow air into the middle ear. They also may be called tympanostomy tubes, myringotomy tubes, ventilation tubes, or PE (pressure equalization) tubes.
These tubes can be made out of various materials and come in two basic types: short-term and long-term. Short- term tubes are smaller and typically stay in place for six to eighteen months before falling out on their own. Long-term tubes are larger and have flanges that secure them in place for a longer period of time. Long-term tubes may fall out on their own, but removal by an otolaryngologist may be necessary. Rosenfeld RM. A Parent’s Guide to Ear Tubes. Hamilton, Ontario, Canada: BC Decker; 2005. Reproduced with permission.
WHO NEEDS EAR TUBES AND WHY? Ear tubes may be recommended when a person experiences repeated middle ear infection (acute otitis media) or has hearing loss caused by persistent middle ear fluid (otitis media with effusion). These conditions most commonly occur in children, but can also be present in teens and adults and can lead to speech and balance problems, hearing loss, poor school performance, or changes in the structure of the ear drum. Other less common conditions that may warrant the placement of ear tubes are malformation of the ear drum or eustachian tube, Down Syndrome, cleft palate, and barotrauma (injury to the middle ear caused by a reduction of air pressure, usually seen with altitude changes as in flying and scuba diving).
Each year, more than half a million ear tube surgeries are performed on children, making it the most common childhood surgery performed with anesthesia. The average age for ear tube insertion is one to three years old. Inserting ear tubes may:
Reduce the risk of future ear infection;
Restore hearing loss caused by middle ear fluid;
Improve speech problems and balance problems; and
Improve behavior and sleep problems caused by chronic ear infections; and
Help children do their best in school.
HOW ARE EAR TUBES INSERTED IN THE EAR? Ear tubes are inserted through an outpatient surgical procedure called a myringotomy. A myringotomy refers to an incision (small opening) in the ear drum or tympanic membrane, which is most often done under a surgical microscope with a small scalpel. If an ear tube is not inserted, the hole would heal and close within a few days. To prevent this, an ear tube is placed in the hole to keep it open and allow air to reach the middle ear space (ventilation).
WHAT HAPPENS DURING SURGERY? Most young children require general anesthesia but some doctors can do this as a brief office procedure. Some older children and adults may also be able to tolerate the procedure without anesthetic. A myringotomy is performed and the fluid behind the ear drum (in the middle ear space) is suctioned out. The ear tube is then placed in the opening. Ear drops may be administered after the ear tube is placed and may be prescribed for a few days. The procedure usually lasts less than 15 minutes and patients recover very quickly.
Sometimes the otolaryngologist will recommend removal of the adenoid tissue (lymph tissue located in the upper airway behind the nose) when ear tubes are placed for persistent middle-ear fluid. This is effective for children four years or older and is often considered when a repeat tube insertion is necessary. Current research indicates that removing adenoid tissue concurrent with placement of ear tubes for persistent middle-ear fluid can reduce the risk of recurrent ear infections and the need for repeat surgery in children four years and older.
WHAT HAPPENS AFTER SURGERY? After surgery, the patient is monitored in the recovery room (if general anesthesia was used) and will usually go home within an hour or two if no complications occur. Patients usually experience little or no postoperative pain, but grogginess, irritability, and/or nausea from the anesthesia can occur temporarily. When done in the office recovery is immediate.
Hearing loss caused by the presence of middle ear fluid is immediately resolved by surgery. Children with speech, language, learning, or balance problems may take several weeks or months to fully improve.
The otolaryngologist will provide specific postoperative instructions, including when to seek attention and to set follow-up appointments. He or she may also prescribe an antibiotic ear drops for a few days. An audiogram should be performed after surgery, if hearing loss is present before the tubes are placed. This test will make sure that hearing has improved with the surgery.
Although the tube does have a small opening (about 1/20th of an inch) that could allow water to enter the middle ear, research studies show no benefit in keeping the ears dry and current guidelines do not recommend routine water precautions. Therefore, you do not need to restrict swimming or bathing while tubes or in place and do not need to use earplugs, head bands, or other water-tight devices unless specifically recommended by your doctor.
POSSIBLE COMPLICATIONS Myringotomy with insertion of ear tubes is an extremely common and safe procedure with minimal complications. When complications do occur, they may include:
Perforation: This can rarely happen when a tube comes out or a long-term tube is removed and the hole in the tympanic membrane (ear drum) does not close. The hole can be patched through a surgical procedure called a tympanoplasty or myringoplasty.
Scarring: Any irritation of the ear drum (recurrent ear infections), including repeated insertion of ear tubes, can cause scarring called tympanosclerosis or myringosclerosis. In most cases, this causes no problem with hearing and does not need any treatment.
Infection: Ear infections can still occur with a tube in place and cause ear discharge or drainage. However, these infections are usually infrequent, do not cause hearing loss (because the infection drains out), and may go away on their own or be treated effectively with antibiotic ear drops. Oral antibiotics are rarely needed.
Ear tubes come out too early or stay in too long: If an ear tube expels from the ear drum too soon (which is unpredictable), fluid may return and repeat surgery may be needed. Ear tubes that remain too long may result in perforation or may require removal by an otolaryngologist.
If your child has tried antihistamines and/or nasal steroids but their symptoms did not improve, the pediatrician may send a referral to a specialist.
Which specialist? An Allergist or an ENT (Ear, Nose and Throat)?
At Ohio ENT & Allergy Physicians, both specialties work together to sort these problems out. At one of our 10 convenient locations, a pediatric patient with chronic nasal and sinus symptoms can be evaluated for both adenoid problems and allergies. Testing will include routine allergy testing, a thorough physical exam and sometimes the use of a small flexible endoscope to evaluate the nasal passages and check the size of the adenoids. This scope also allows diagnosis of other problems such as a nasal foreign body, a polyp, or a deviated nasal septum (which is rare in children).
Medical treatment may be tried again by our specialists. This may include stronger nasal sprays, antihistamines, antibiotics or allergy shots (immunotherapy).
If this treatment is still not effective, surgical treatment may be offered. This may include removal of the adenoids and treatment of the nasal swellings called “turbinates”. Sometimes tonsillectomy or ear tube insertion may be necessary, as well. (These will be discussed in a future blog.)
These surgeries would likely be done at The Ohio Surgery Center, an accredited, outpatient surgery center staffed by anesthesiologists and nurses with extensive pediatric experience and training. The recovery is usually quite fast with minimal discomfort.
Though up to 90% of children will be effectively treated by addressing allergies and adenoid problems, a small number will continue to have problems. This is where it is extremely beneficial to have the two specialists working together. The allergist will look for more unusual allergies including food allergies or asthma and check the patient’s immune system to make sure it is working properly. The ENT doctors will look for nasal problems such as polyps or chronic sinus infections, utilizing a very low radiation office CAT scanner, when necessary. Having the CAT scan done in the office allows for a convenient “less scary” seated CAT scan (similar to a dental X-RAY). An office scan is also much less expensive than a hospital scan.
A child with a cold is not a pleasant experience. But a cold that never goes away is a sign of a medical problem that requires further evaluation. Once the cause has been determined effective treatment can be offered. This may require allergy treatment, treatment for enlarged adenoids or both.
At Ohio ENT & Allergy Physicians, we have specialists to deal with both allergy problems and adenoid problems in a convenient outpatient setting and in a cost-effective manner.
 Some people react to particles in the air. These particles, called “allergens” include pollen from various plants, dust, mold or pet dander. Allergies occur when the allergens are inhaled into the respiratory tract of allergic people. The particles cause cells in the nose to release histamine, which then leads to the symptoms of sneezing, running nose and nasal congestion. Some patients wheeze from asthma — asthma and rashes are sometimes related to allergies. Allergies can be seasonal or year-round depending on what the patient is allergic to.
Some people react to particles in the air. These particles, called “allergens” include pollen from various plants, dust, mold or pet dander. Allergies occur when the allergens are inhaled into the respiratory tract of allergic people. The particles cause cells in the nose to release histamine, which then leads to the symptoms of sneezing, running nose and nasal congestion. Some patients wheeze from asthma — asthma and rashes are sometimes related to allergies. Allergies can be seasonal or year-round depending on what the patient is allergic to.